Laser Genesis Consent Form

Laser Hair Removal Is A Medical Procedure Of Hair Removal That Stops The Hair Growth Permanently New Dawn Med Spa Has Laser Hair Removal Hair Removal Med Spa

Got Big Pores Laser Genesis For Pore Size Texture Sholarcenter Skin Rejuvenation Improve Skin Texture Laser Skin

Patient Forms Turquoise Springs Medical Spa

Skin Treatments Forget Me Not Day Spa Facial Room Spa Facial Room Esthetician Room

Laser Genesis Cosmetic Dermatology Dermatologists In San Antonio

Laser Genesis

I understand that this procedure works on promoting vibrant and healthy looking skin by creating a thermal response in the dermis that.
Laser genesis consent form. I hereby authorize the staff at the re be skin clinic to perform laser genesis non ablative skin therapy on me. Hippa form health history consult financial and cancellation policy consent forms. I understand that this procedure works on promoting vibrant and healthy looking skin by creating a thermal response in the dermis that stimulates new collagen. Physicians using this template are responsible.
Patient informed consent form template for laser genesis skin therapy note. That you carefully review this procedural consent form and ask any questions necessary to help you fully understand it. Patient consent form for laser genesis skin therapy patient client name. Buffalo wy 82834 307 684 2228 i hereby authorize under dr s supervision to perform genesis non ablative skin therapy on me.
Roland fuertez or employees under dr. I understand that this procedure works on promoting vibrant and healthy looking skin. Vein treatment consent hair laser removal consent skin titan consent laser genesis consent pigmented lesions consent dermal filler consent botox dysport xeomin consent form kybella consent form zerona consent form. I understand that this procedure works on.
Proven results in a split face side by side clinical study published in the journal dermatologic surgery the 532 nm ktp laser system was at least as effective as if not more than the 595 nm pulsed dye laser in all study participants with facial. Bartlett or any delegated associates to perform laser genesis non ablative skin therapy on me. Mechanism laser genesis is a non ablative laser procedure to improve skin texture and firmness targeting the papillary dermis. The nd yag is also utilized to perform cutera s signature laser genesis procedure.
Patient consent form for laser genesis skin therapy name. Patient informed consent form for genesis skin therapy laser genesis genesisv genesisplus family medical center of johnson county 497 w. Patient informed consent form for laser genesis skin therapy i hereby authorize dr. I hereby authorize and direct any associates of novas dohr coll ob gyn associates medical spa to perform laser genesis non ablative skin therapy on me.
Please sign only after careful review and consideration. This patient informed consent template is provided as is and is intended for informational purposes only. This template may not meet all state and federal legal or regulatory requirements for use with patients.

Laser Hair Reduction Cosmetic Dermatology Dermatologists In San Antonio

Client Record Card Pagehtm Esthetician Esthetics Beauty Business

D5keodtj1 Qelm

Sequential Facial Skin Rejuvenation With Intense Pulsed Light And Non Ablative Fractionated Laser Resurfacing In Fitzpatrick Skin Type Ii Iv Patients A Prospective Multicenter Analysis Knight 2019 Lasers In Surgery And

Laser Genesis Encinitas Ca Pore Minimizer Treatments

Laser Treatments Medical Spa Springfield Clinic

Laser Genesis Reviews Blog Prescott Medical Aesthetics

Mexican Marriage Certificate Template Awesome Marriage Certificate In 2020 Marriage Certificate Certificate Templates Marriage

Wowder Duo With Images Glossier Wowder Wowder

Tattoo Removal Results Enlighten Aesthetic Cleveland Tattoo Removal Results Tattoo Removal Tattoos

Kevin Cease Aging Skin Comparison Cosmetic Injectables Skin Healing Facial Skin Care
Laser Genesis Skin Treatment Vein And Laser Institute

What Symptoms Does The Laser Genesis Treatment Target Laser Genesis Laser Skincare

Laser Rejuvenation Results Enlighten Aesthetic

Skin Revitalization Resurfacing Cedar Rapids Ia Cosmetic Solutions Laser And Skin Care Center

Endymed Intensif Rf Microneedle Union Square Laser Dermatology

Laser Genesis Pore Reduction And Skin Rejuvenation

Noul Univers Christalin 9 Crăciunul Ca Zi A Nasterii Domnului Hristos Ethereal Art Ascended Masters Visionary Art
Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gctw4672dp11j2u Vd Hyjxf7xdkkpzjecaarnegk3o Usqp Cau

Laser Genesis Large Pores Tamra Bedford Cosmetic Rn Laser Hair Removal

Pdf Low Level Laser Therapy For The Patients With Painful Diabetic Peripheral Neuropathy A Systematic Review
Pdf Lsm W 2 Laser Scanning Microscopy Worker For Wheat Leaf Surface Morphology

Laser Genesis Prescott Medical Aesthetics

Cnc 051 Dekupe Kapak Market Cnc Isleme Mobilya Teknoloji Cnc Mobilya Dekor

Pin On Injectable Fillers By Dr Kim
Ipl Photofacial Los Angeles Redondo Beach

How Effective Is Picosure Laser For Melasma Removal Clearifirx Blog

Laser Treatments Keller Dallas Fort Worth Texas

Ipl Photofacial Prescott Medical Aesthetics
Https Academic Oup Com Jcem Article Pdf 91 9 3633 9065494 Jcem3633 Pdf
U S Laws For Lasers And Pointers

New Clients Hospitality Medical Aesthetics

Skin Lasers Laser Services Treatments Drs Tripti Burt Neena Will

Laser Skin Tightening Precision Aesthetics Medical Group Cosmetic Specialists Orange County Ca
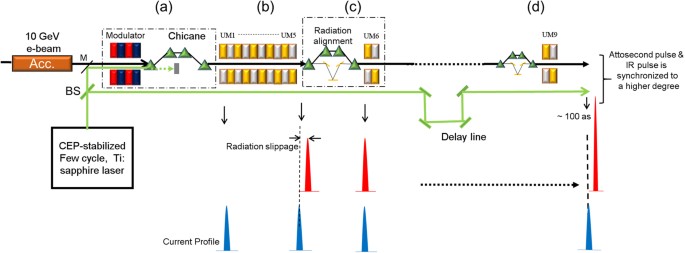
Temporally Coherent Terawatt Attosecond Xfel Synchronized With A Few Cycle Laser Scientific Reports

Pin On Inspirations For Midterm
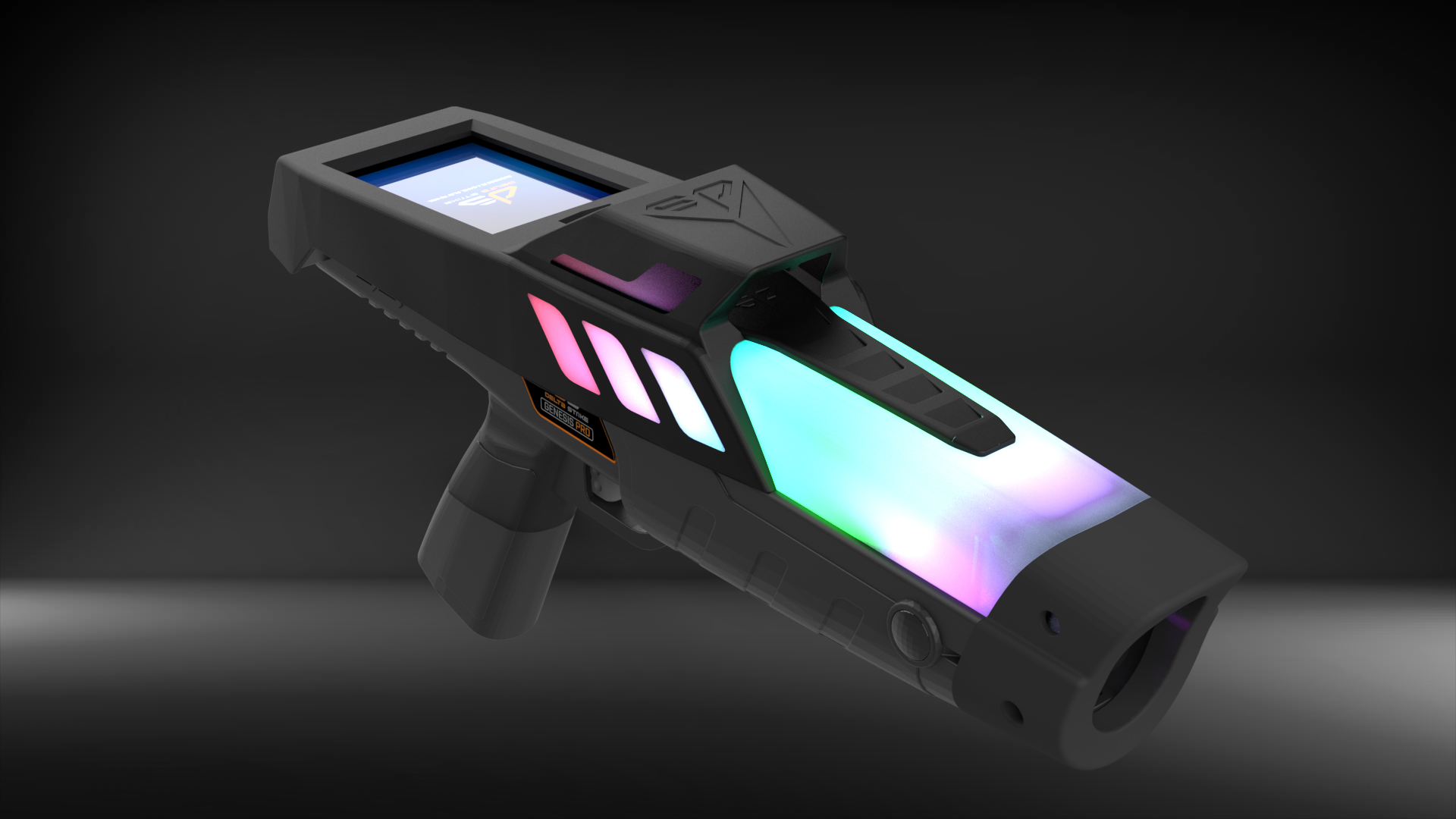
Delta Strike Laser Tag December 2019 Replay Magazine
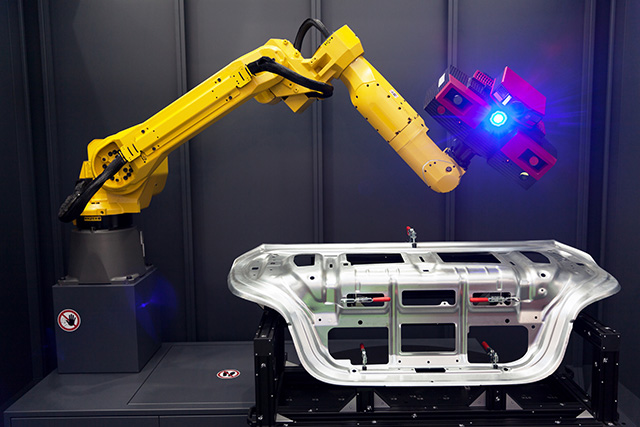
Laser Brazing For Material Removal In Aerospace Manufacturing

What Is Laser Shearography Non Destructive Inspection And How Is It Used In Aerospace

Laser Hair Removal Orange County Ca Laser Hair Removal Near Me

Best Laser Hair Removal Blog Prescott Medical Aesthetics